
The Richland Hospital, Inc. - Richland Center, 2026 Quality
Improving Medication Management and Safety Through Pharmacist Led Initiatives
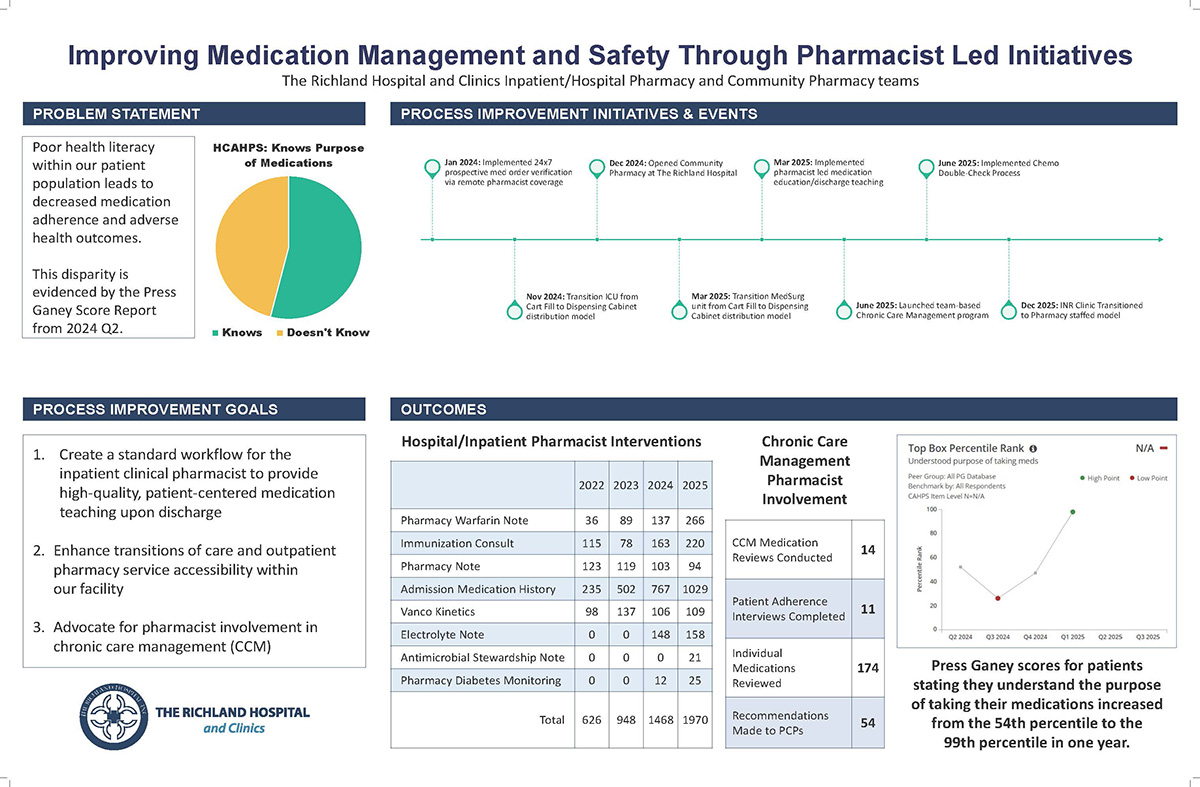
Medication management is a cornerstone of safe, effective healthcare, yet poor health literacy and fragmented transitions of care can significantly undermine patient outcomes. At The Richland Hospital and Clinics, we identified an opportunity to improve medication understanding, adherence, and safety through intentional expansion of pharmacist-led initiatives across inpatient, outpatient, and chronic care settings. This work was driven by both patient experience data and frontline observations that underscored the impact pharmacists can have when fully integrated into the care team.
Our journey began with a challenge. Press Ganey results from Q2 2024 showed that patients’ understanding of the purpose of their medications lagged behind benchmarks, highlighting a disparity that placed patients at risk for adverse outcomes. Recognizing that medication education and access are inseparable from quality care, we established three core improvement goals: standardizing pharmacist-led discharge education, strengthening transitions of care with enhanced outpatient pharmacy access, and expanding pharmacist involvement in chronic care management (CCM).
Over a two-year period, we implemented a series of coordinated process improvements to support these goals. In January 2024, we introduced 24/7 prospective medication order verification through remote pharmacist coverage, improving real‑time safety and oversight. This was followed by transitioning both ICU and Med/Surg units from cart fill to dispensing cabinet distribution models, increasing accuracy, efficiency, and access at the point of care.
A major milestone occurred in December 2024 with the opening of our on‑site Community Pharmacy. This advancement significantly improved continuity of care, enabling patients to leave the hospital with immediate access to medications and direct pharmacist counseling. In March 2025, we strengthened this work by implementing pharmacist-led medication education and discharge teaching, ensuring that patients clearly understood the purpose, dosing, and follow‑up associated with their medications.
Pharmacist involvement continued to expand beyond discharge. In June 2025, we launched a team‑based Chronic Care Management program, formally integrating pharmacists into longitudinal care. Within the first phase alone, pharmacists conducted 14 CCM medication reviews, completed 11 patient adherence interviews, reviewed 174 individual medications, and made 54 recommendations to primary care providers. These interventions helped identify duplications, adherence barriers, therapeutic gaps, and opportunities for safer, more effective regimens.
Additional safety‑focused initiatives—including a chemotherapy double‑check process and the transition of the INR Clinic to a pharmacy‑staffed model—further broadened the scope of pharmacist contributions. Collectively, these efforts resulted in a substantial increase in documented pharmacist interventions across inpatient care, from admission medication histories and warfarin monitoring to antimicrobial stewardship and diabetes oversight.
The outcomes of this work have been both measurable and meaningful. Within one year, Press Ganey scores for patients who reported understanding the purpose of their medications rose from the 54th percentile to the 99th percentile—an extraordinary improvement that reflects the power of patient‑centered education and consistent engagement. HCAHPS data further reinforced gains in medication understanding, highlighting the sustained impact of embedding pharmacists across care transitions.
This initiative demonstrates that pharmacists are not ancillary contributors but essential partners in delivering high‑quality, patient‑centered care. By aligning medication safety, education, and access through structured workflows and interdisciplinary collaboration, we have strengthened both patient experience and clinical outcomes.
Our journey began with a challenge. Press Ganey results from Q2 2024 showed that patients’ understanding of the purpose of their medications lagged behind benchmarks, highlighting a disparity that placed patients at risk for adverse outcomes. Recognizing that medication education and access are inseparable from quality care, we established three core improvement goals: standardizing pharmacist-led discharge education, strengthening transitions of care with enhanced outpatient pharmacy access, and expanding pharmacist involvement in chronic care management (CCM).
Over a two-year period, we implemented a series of coordinated process improvements to support these goals. In January 2024, we introduced 24/7 prospective medication order verification through remote pharmacist coverage, improving real‑time safety and oversight. This was followed by transitioning both ICU and Med/Surg units from cart fill to dispensing cabinet distribution models, increasing accuracy, efficiency, and access at the point of care.
A major milestone occurred in December 2024 with the opening of our on‑site Community Pharmacy. This advancement significantly improved continuity of care, enabling patients to leave the hospital with immediate access to medications and direct pharmacist counseling. In March 2025, we strengthened this work by implementing pharmacist-led medication education and discharge teaching, ensuring that patients clearly understood the purpose, dosing, and follow‑up associated with their medications.
Pharmacist involvement continued to expand beyond discharge. In June 2025, we launched a team‑based Chronic Care Management program, formally integrating pharmacists into longitudinal care. Within the first phase alone, pharmacists conducted 14 CCM medication reviews, completed 11 patient adherence interviews, reviewed 174 individual medications, and made 54 recommendations to primary care providers. These interventions helped identify duplications, adherence barriers, therapeutic gaps, and opportunities for safer, more effective regimens.
Additional safety‑focused initiatives—including a chemotherapy double‑check process and the transition of the INR Clinic to a pharmacy‑staffed model—further broadened the scope of pharmacist contributions. Collectively, these efforts resulted in a substantial increase in documented pharmacist interventions across inpatient care, from admission medication histories and warfarin monitoring to antimicrobial stewardship and diabetes oversight.
The outcomes of this work have been both measurable and meaningful. Within one year, Press Ganey scores for patients who reported understanding the purpose of their medications rose from the 54th percentile to the 99th percentile—an extraordinary improvement that reflects the power of patient‑centered education and consistent engagement. HCAHPS data further reinforced gains in medication understanding, highlighting the sustained impact of embedding pharmacists across care transitions.
This initiative demonstrates that pharmacists are not ancillary contributors but essential partners in delivering high‑quality, patient‑centered care. By aligning medication safety, education, and access through structured workflows and interdisciplinary collaboration, we have strengthened both patient experience and clinical outcomes.
